Physical therapy marketing should create booked evaluations, attended visits and completed plans of care, not just cheap calls. A clinic rarely wins on one isolated appointment. The commercial value usually sits in the full care episode: an initial evaluation, a treatment plan, follow-up visits, reactivations and referrals from satisfied patients.

That changes the marketing model. A campaign can look efficient when it reports a low cost per click, yet fail commercially if calls are unqualified, insurance is unclear, direct-access questions are unanswered or the clinic never receives feedback from the schedule and billing system. Strong physical therapy marketing joins local search intent, clinical trust signals, privacy-safe tracking and a sales process that moves people from research to evaluation.
This article is the English-market counterpart of our Polish guide to advertising a physiotherapy practice. The core principle is the same - measure real appointments and patient value - but the operating context is different: state-level direct access rules, payer mix, HIPAA considerations, Google and Meta health-ad policies, and a much stronger need to distinguish insurance-based care from cash-pay positioning.
TL;DR
- The best metric is cost per qualified new patient. Calls and forms are early signals; attended evaluations and plans of care show business value.
- Google Search captures the highest intent. Local, condition, post-op, specialty and insurance/direct-access searches need separate structure.
- Google Business Profile often decides trust. Reviews, photos, location, hours, booking links and services affect whether a researcher becomes a patient.
- Direct access is a major education angle. APTA states that all US states, Washington DC and the US Virgin Islands have provisional or unrestricted direct access, but rules and payer requirements still vary.
- Insurance and cash-pay clinics need different messages. Coverage, convenience and network access are different from specialization, time, speed and experience.
- Healthcare tracking has to be privacy-safe. Platforms should receive neutral conversion events, not condition details, treatment notes or protected health information.
Why Physical Therapy Marketing Is Different
Physical therapy sits between local services, healthcare, referral relationships and patient education. That combination makes generic lead-generation playbooks weak.
First, demand is local and problem-led. Searchers use phrases such as "physical therapy near me," "sports physical therapy [city]," "physical therapy after knee replacement," "pelvic floor PT," "vestibular physical therapist" or "PT that accepts [insurance]." Each phrase implies a different question. A generic home page cannot answer all of them well.
Second, trust is part of the conversion. Patients compare reviews, credentials, location, parking, availability, accepted insurance, photos of the clinic and whether the practice explains the next step clearly. In healthcare, a frictionless form is not enough. The clinic also has to feel competent, legitimate and easy to contact.
Third, the value is episode-based. A booked evaluation is valuable, but the real economics depend on show rate, payer, authorized visits, plan completion, add-on services, reactivation and referrals. A campaign optimized only for "call started" can overfund low-quality demand and underfund channels that create higher-value patients.
Fourth, advertising and tracking operate under healthcare constraints. Google restricts several healthcare and medicines categories, Google personalized advertising rules limit use of sensitive health signals, Meta has health and wellness ad standards, and HIPAA governs how protected health information can be used in marketing. This is not a legal interpretation; it is a practical reminder that the measurement plan should be reviewed against local laws, payer rules and platform policies before launch.
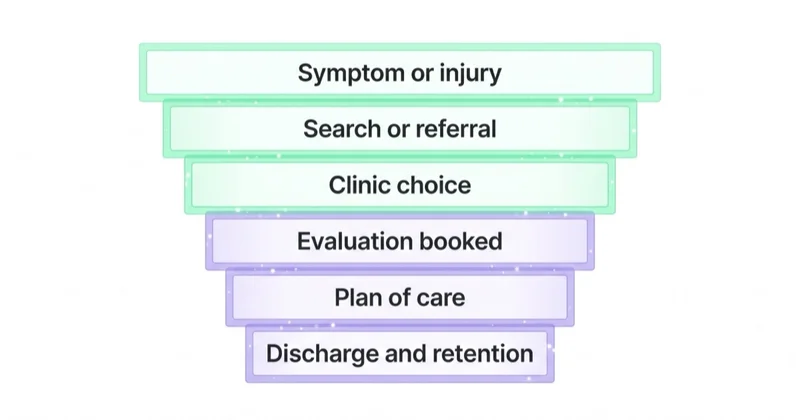
The Patient Journey
Most physical therapy funnels are not linear. A patient may hear about a clinic from a surgeon, search the clinic name, read reviews, check insurance, compare appointment availability, ask whether a referral is required and call later from a mobile device. The campaign only gets credit if tracking is built around that reality.
| Stage | Patient Question | Marketing Asset |
|---|---|---|
| Problem recognition | "Can PT help with this situation?" | Condition or specialty page with neutral education |
| Local comparison | "Which clinic near me looks credible?" | Google Business Profile, reviews, photos, hours |
| Access check | "Is a referral required? Is insurance accepted?" | Direct-access and insurance information |
| Booking | "How fast can an evaluation be scheduled?" | Clear booking CTA, phone, form, location |
| Care episode | "Will this plan fit my life?" | Appointment reminders, plan communication, reactivation |
The practical goal is to reduce uncertainty before the call. If the website and ads answer access, insurance, specialty and booking questions, the front desk spends less time filtering poor-fit inquiries and more time scheduling qualified evaluations.
Channel Mix for Physical Therapy Clinics
| Channel | Best Role | Main Risk |
|---|---|---|
| Google Search | Capturing local, condition, post-op and specialty intent | One generic campaign wastes spend on mixed intent |
| Google Business Profile | Local trust, Maps visibility, reviews, calls and directions | Thin profile lowers conversion even when ads work |
| Meta / Instagram | Education, awareness, reactivation and specialty positioning | Health-policy issues if copy implies a viewer's condition |
| Referral marketing | Surgeons, physicians, trainers, employers and community partners | Offline value is lost without CRM tracking |
| Email / SMS / CRM | Reactivation, plan completion and no-show reduction | Consent and privacy controls must be documented |
The general local framework is covered in Google Ads for local businesses. Physical therapy needs the same local discipline, then adds healthcare language, payer segmentation, direct-access education and privacy-safe offline feedback.
Google Search Structure
Search is usually the highest-intent paid channel because it captures people already looking for help, access or a specific service. The structure should separate the major demand types instead of placing every keyword in one ad group.
| Intent | Example Queries | Landing Page Need |
|---|---|---|
| Local | "physical therapy near me," "physical therapist [city]" | Location, hours, reviews, insurance, booking |
| Condition | "back pain physical therapy," "sciatica PT" | Neutral education, evaluation CTA, clinician expertise |
| Post-surgical | "physical therapy after ACL surgery," "knee replacement rehab" | Post-op coordination, timelines, physician collaboration |
| Specialty | "sports physical therapy," "pelvic floor therapist," "vestibular rehab" | Specialty credentials, services, privacy-sensitive copy |
| Access / payer | "PT without referral," "physical therapy that takes [insurer]" | Direct-access rules, accepted plans, verification steps |
| Branded | Clinic name, clinician name, competitor comparisons | Trust protection, review proof, direct booking |
Negative keywords matter. Many searches around physical therapy are not commercial clinic demand: salary, school, jobs, exercises, stretches, PDF, certification, free, at home, equipment, textbook and continuing education. Without exclusions, budget can drift into research, employment and DIY traffic.
Landing pages should match the query. A post-op keyword should not send a patient to a generic services page. A pelvic health query needs careful, private language and clear clinician expertise. An insurance query needs coverage guidance and a path to verification. Relevance improves both conversion and the likelihood that AI search systems can understand what the clinic is actually known for.
Direct Access: High-Value Education, Not a Throwaway Line
Direct access is one of the most important differences in US physical therapy marketing. APTA states that, as of July 1, 2025, all 50 states, Washington DC and the US Virgin Islands have either provisional or unrestricted direct access to physical therapist services for evaluation and treatment. That does not mean every patient can receive unlimited care without conditions. State rules, payer requirements, visit limits and referral provisions still vary.
For marketing, that nuance matters. The strongest message is not a blanket promise. It is a clear explanation:
- an evaluation may be available without a physician referral;
- the clinic can explain state and payer requirements before scheduling;
- insurance verification may still be required;
- some plans or treatment durations may require referral, authorization or documentation;
- the clinic coordinates with physicians when clinically appropriate.
This turns a common patient objection into a booking asset. Many people delay care because they assume a referral is the first step. A direct-access page, direct-access ad group and FAQ can shorten the path from search to evaluation while staying factual.
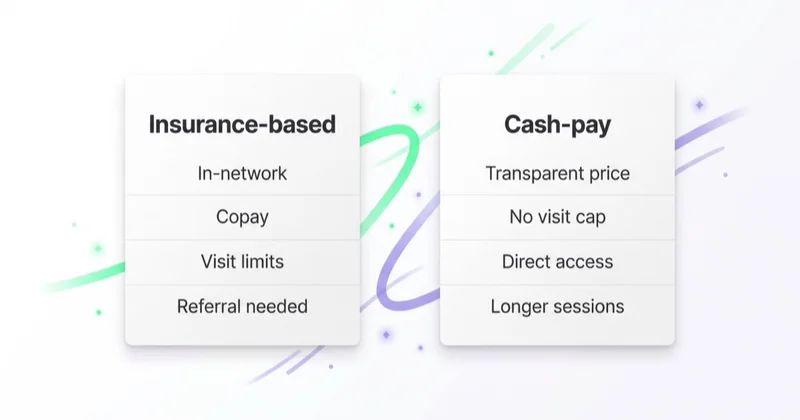
Insurance vs Cash-Pay Positioning
Physical therapy clinics do not all sell the same decision. Insurance-based, cash-pay and hybrid clinics need different language, landing pages and reporting.
| Model | What Converts | Measurement Focus |
|---|---|---|
| Insurance / in-network | Accepted plans, convenience, access, verification, appointment availability | New patients by payer, authorized visits, plan completion |
| Cash-pay / out-of-network | One-on-one time, specialization, experience, speed, continuity | Evaluation value, package value, retention, referral value |
| Hybrid | Clear routing between insurance and private-pay paths | Cost per patient by segment, not blended averages |
Insurance-based clinics should make coverage easy to verify without overpromising benefits. Cash-pay clinics have to justify value before price becomes the only comparison. Hybrid clinics need separate paths so a patient searching "PT that takes Blue Cross" is not reading the same page as a self-pay runner looking for sports performance work.
Blended reporting hides problems. A clinic can have a healthy average cost per lead while one payer segment is unprofitable and one specialty is underfunded. Reporting by payer model, location, specialty and plan-of-care value gives management a much cleaner view.
Google Business Profile and Local Trust
Google Business Profile is not a directory afterthought. For a local clinic, it often acts as the second landing page. A searcher may click an ad, return to Maps, read reviews, compare photos and call from the profile rather than the website.
For physical therapy, the profile should include:
- accurate primary and secondary categories;
- current hours for every location;
- correct phone numbers, appointment links and UTM-tagged website links;
- photos of the exterior, reception, treatment areas, equipment and team;
- service listings that reflect real specialties;
- recent reviews and professional responses;
- clear location details such as parking, accessibility and nearby landmarks.
Review responses need special discipline. A response should not confirm that someone is a patient, mention a condition, reference treatment details or discuss outcomes. General, courteous language protects trust without exposing sensitive information.
Local SEO should reinforce the same entity signals. Location pages, specialty pages, clinician bios, FAQ content, schema where appropriate and consistent NAP data help both search engines and AI systems connect the clinic with its services, locations and expertise.
Condition and Specialty Pages
Condition and specialty pages are useful only when they are specific, careful and clinically credible. Thin pages that repeat "physical therapy for pain" across twenty URLs create little value. Better pages answer the questions that shape a booking decision:
- what type of patient or situation the page is for;
- what the evaluation typically covers;
- which clinicians or credentials are relevant;
- what referral, insurance or direct-access steps may apply;
- what to bring to the first visit;
- how scheduling works;
- when the clinic will coordinate with a physician or surgeon.
The language should stay neutral. Ads and pages can describe services for back pain, post-surgical rehabilitation, pelvic health, sports injury, balance, vestibular care or workplace injury without declaring that a specific viewer has a condition. This matters for both conversion quality and platform policy.
High-value pages also support AEO and LLM visibility. AI systems tend to extract direct answers from pages that include clear service definitions, eligibility context, location details, FAQs, clinician expertise and structured next steps.
Meta, Instagram and Education
Meta is rarely the best channel for urgent "PT near me today" demand. It is useful for education, awareness, reactivation and specialty positioning when the copy is compliant.
Strong Meta angles include:
- direct-access education without implying a viewer's condition;
- specialty explainers for sports PT, pelvic health, vestibular care or post-op rehab;
- clinician introductions and facility walkthroughs;
- community partnerships with gyms, running clubs, employers or sports teams;
- reactivation campaigns to past patients where consent and policy allow;
- content that explains evaluation, insurance verification and booking steps.
Weak Meta angles include before/after claims, fear-based pain copy, over-personalized wording and promises of outcomes. Copy such as "Still dealing with your knee pain?" creates policy and trust risk because it points a health condition at the viewer. A safer version is "Physical therapy appointments for knee and post-surgical rehabilitation in [city]."
The same care applies to retargeting. Healthcare-advertising rules can restrict advertiser-curated audiences and sensitive health signals. When in doubt, use broader local education, neutral creative and consented CRM communication instead of narrow health-condition audiences.
Referral Marketing and Community Demand
Paid media does not replace relationships in physical therapy. Surgeons, primary care physicians, orthopedists, employers, athletic trainers, coaches, gyms and previous patients can all drive qualified demand. The issue is that many clinics treat referral demand as unmeasured "word of mouth."
A practical referral system includes:
- source fields in the CRM or practice-management system;
- unique landing pages or call tracking for partner campaigns where appropriate;
- monthly reporting by referrer, specialty, payer and plan completion;
- patient education materials that partners can use;
- events or workshops that create local authority without exaggerated claims.
The goal is not to force every referral through paid attribution. The goal is to see which relationships create attended evaluations and completed care episodes, then support those channels with the right content and follow-up.
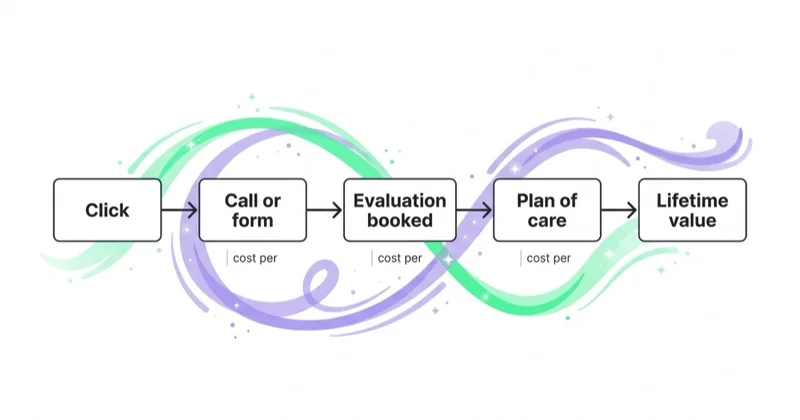
Measurement: From Lead to Plan of Care
Physical therapy accounts often fail because the platform optimizes to the wrong event. A call is not a patient. A form is not an attended evaluation. A booked evaluation is not a completed plan of care.
| Event | Meaning | Use in Optimization |
|---|---|---|
call_started |
A phone interaction from an ad or profile | Early diagnostic signal |
form_submitted |
A digital inquiry | Early diagnostic signal |
evaluation_booked |
New-patient evaluation scheduled | Primary lead-quality signal |
evaluation_attended |
Patient arrived for evaluation | Strong optimization signal |
plan_of_care_started |
Treatment plan began | Value signal |
plan_completed |
Care episode completed | Business-quality signal |
reactivation |
Past patient returned | Lifetime-value signal |
Google call reporting and offline conversion imports can connect calls, booked evaluations and later outcomes back to ad interactions. The privacy line is important: send neutral event names and values, not diagnosis, treatment notes, insurer details, appointment notes or other protected health information. Intake, clinical records and billing data belong in appropriate healthcare systems, not in ad-platform tags.
Call tracking also deserves nuance. More calls are not always better. Calls need duration filters, source context, front-desk notes and outcome labels. A five-second wrong-number call should not carry the same value as a scheduled evaluation.
How Space Ads Approaches Physical Therapy Accounts
For physical therapy, the Space Ads approach starts with patient economics and operational reality. The first questions are not about bids. They are about the clinic's value model: locations, specialties, payer mix, evaluation capacity, show rate, average visits per plan, plan completion, reactivation and referral sources.
Only then does channel structure make sense. Google Search captures local and condition intent. Google Business Profile improves trust and conversion. Meta supports education and reactivation when privacy and platform rules allow. Referral campaigns are measured through CRM outcomes. Reporting focuses on cost per attended evaluation, cost per plan of care and value by specialty or payer segment.
For clinics already spending on ads, a marketing audit should find whether the account is producing patients or merely generating calls. Ongoing execution can combine Google Ads, Meta Ads and performance marketing, but only after tracking and patient-routing logic are clean enough to guide budget.
30-Day Improvement Plan
- Days 1-3: map patient economics. Separate locations, specialties, payer mix, evaluation capacity, show rate, plan-of-care value and reactivation value.
- Days 4-7: clean privacy-safe tracking. Track calls, forms, evaluations booked and attended, plans started, plans completed and reactivations with neutral events.
- Days 8-11: strengthen Google Business Profile. Update categories, hours, booking links, photos, services, review responses and location details.
- Days 12-17: rebuild Search structure. Separate local, condition, post-op, specialty, insurance and direct-access intent; add negative keywords.
- Days 18-22: improve landing pages. Build pages for the highest-value services with clinician proof, access guidance, insurance context and booking CTAs.
- Days 23-26: add Meta education carefully. Use direct-access, facility, specialty and clinician content without over-personalized health claims.
- Days 27-30: review by attended outcomes. Compare sources by attended evaluation, plan-of-care value and payer/specialty quality, not clicks.
Common Mistakes
| Mistake | Better Approach |
|---|---|
| Optimizing only for calls | Import attended evaluations and plan-of-care events |
| One campaign for every service | Split by local, condition, post-op, specialty and payer intent |
| Treating direct access as a footnote | Build a factual direct-access page and ad group |
| Blending insurance and cash-pay audiences | Segment messages, pages and reporting |
| Sending sensitive data to ad platforms | Use neutral conversion events and privacy-safe workflows |
| Ignoring Google Business Profile | Treat the profile as a conversion page with reviews and photos |
| Writing vague condition pages | Provide specific, careful, clinically credible answers |
FAQ
What is the most important metric in physical therapy marketing?
Cost per attended new-patient evaluation measured against plan-of-care value is usually more useful than cost per click, cost per form or cost per call. A call can be unqualified, a form can go unanswered and an evaluation can no-show. Attended evaluations, treatment plans, plan completion and reactivation show which channels create real business value.
Does direct access help physical therapy marketing?
Yes, when it is explained accurately. APTA states that all US states, Washington DC and the US Virgin Islands have provisional or unrestricted direct access to physical therapist services for evaluation and treatment. Marketing should still avoid blanket promises because state provisions, payer rules, visit limits and referral requirements can vary. The useful message is that an evaluation may be available without a referral and the clinic can explain the next step.
How should insurance-based and cash-pay PT clinics market differently?
Insurance-based clinics usually convert on accepted plans, convenient access, location, speed and verification. Cash-pay clinics have to communicate specialization, one-on-one time, continuity, experience and value. Hybrid clinics need separate campaigns and pages so payer-driven demand is not mixed with private-pay positioning in one generic message.
Can physical therapy clinics use Meta Ads?
Yes, but Meta works best for education, awareness, specialty positioning and reactivation rather than urgent high-intent search. Copy and creative should stay neutral, avoid declaring a viewer's health condition, avoid fear-based language and respect health-advertising standards. Direct-access education, clinician introductions, facility walkthroughs and local community content are usually safer than over-personalized pain claims.
How can PT marketing stay HIPAA-aware?
Keep protected health information out of ad platforms. Conversion imports should use neutral events such as "evaluation booked" or "plan of care started," not condition details, treatment notes, insurance information or clinical comments. Intake and clinical records should remain in appropriate healthcare systems, and legal or compliance teams should review how marketing data is collected, stored and shared.
What pages does a physical therapy website need for SEO and AEO?
Most clinics need strong location pages, a clear appointment page, insurance and direct-access information, clinician bios, reviews or testimonials handled carefully, and pages for high-value specialties or conditions. Each page should answer practical booking questions: who the service is for, what the first evaluation involves, how scheduling works, which access rules may apply and what information the patient should prepare.
In Short
- Physical therapy marketing should optimize for attended evaluations and plans of care, not clicks.
- Google Search, Google Business Profile and reviews carry the highest local intent.
- Direct access is a valuable education angle when state and payer nuance is preserved.
- Insurance, cash-pay and hybrid clinics need different campaigns, pages and reporting.
- Meta can support education and reactivation, but healthcare copy must stay neutral.
- Measurement should import neutral events and keep health data out of ad platforms.
Sources
- APTA - Direct Access Advocacy
- Google Ads Help - Healthcare and medicines policy
- Google Ads Help - Restricted targeting in Personalized advertising
- Google Ads Help - About call reporting
- Google Ads Help - About offline conversion imports
- Google Business Profile Help - Improve local ranking on Google
- Meta Transparency Center - Health and Wellness ad standards
- HHS - HIPAA marketing guidance
Continue Learning
Continue reading

Wedding Venue Marketing: Tours, Dates and Signed Bookings
Wedding venue marketing should fill the calendar with qualified tours and signed bookings, not just raw inquiries. This guide covers Google Search, Google Business Profile, wedding marketplaces, Instagram, Pinterest, galleries, off-peak dates, CRM follow-up and measuring tour-to-booking value.

Optometry Marketing: Eye Exams, Optical Retail and Patient Value
Optometry marketing should fill the exam schedule, increase optical capture and grow recurring patient value without exposing health data to ad platforms. This guide covers Google Search, local trust, retail eyewear, specialty services, recall and privacy-safe measurement.

Auto Repair Shop Marketing: Google Ads, Local Trust and Booked Bays
Auto repair shop marketing works when local search intent, Google Business Profile, call tracking, service pages, reviews and repair-order value all point to the same outcome: booked bays and profitable repeat customers.